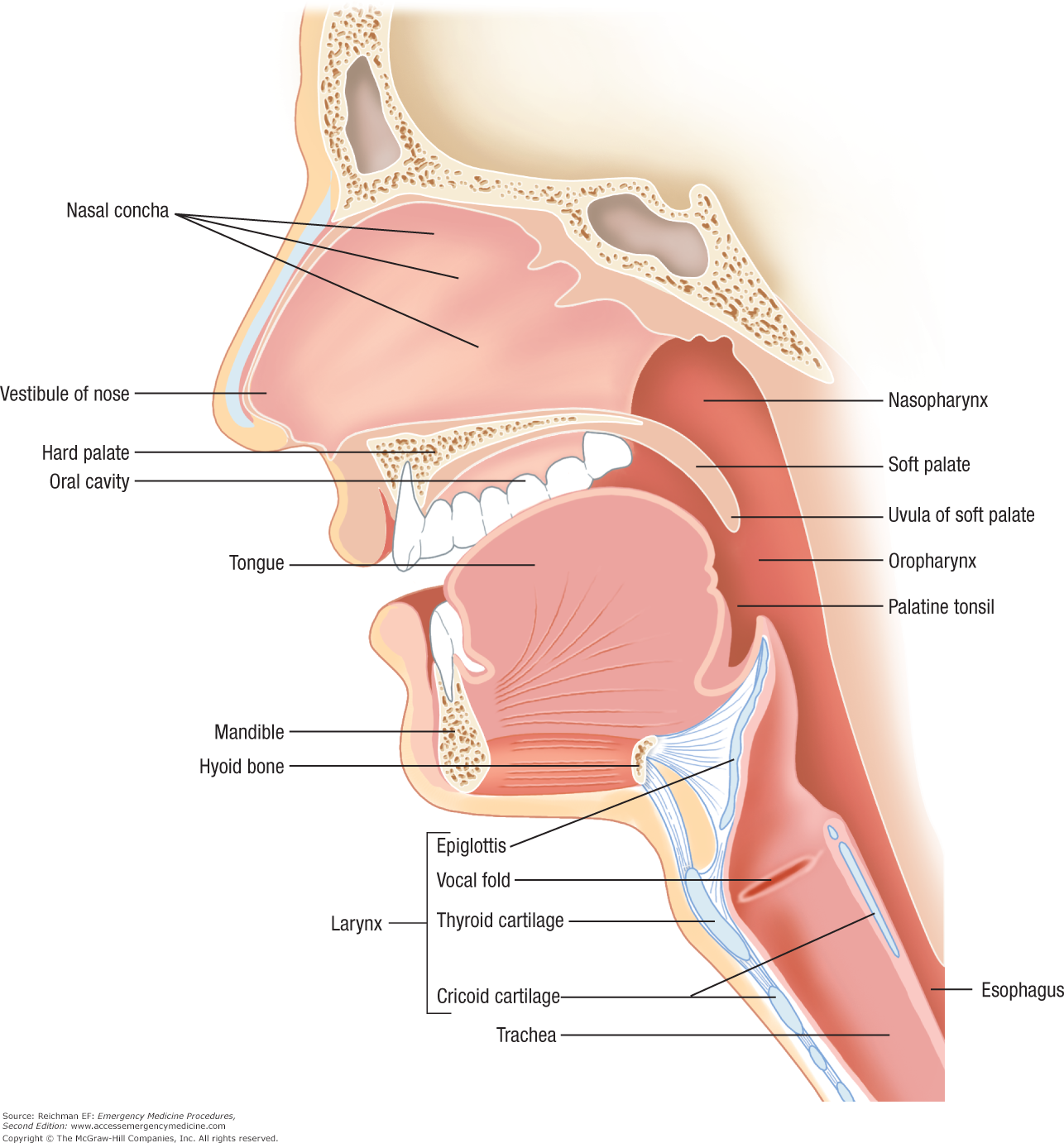
 Click to see larger version! Click to see larger version! Anatomy of the Airway The airway begins at the mouth and nose, which is also referred to as the nasopharynx and oropharynx. These act as the orifices that allow air to enter the lungs. For most of us we breath through our nose, where the nasal concha humidify and filter the air as a protective mechanism. The nasopharynx and oropharynx join at the back of the mouth to form the larynx. The larynx includes important structures such as the epiglottic, vocal cords, and the beginning of the trachea. Also at the back of the larynx is the oesophagus. Bag - Valve Mask The bag-valve mask, also referred to as an ambu bag, is a hand held device that provides positive pressure ventilation to patients who are apneic or not breathing effectively. The ambu bag is a rigid bag that does not require an oxygen/air flow to inflate and provide ventilation, this type of bag-valve mask is best suited to emergency situations. In anaesthesia we commonly use a Mapleson C circuit which consists of a flaccid bag, PEEP valve, oxygen inlet and a mask. The purpose of the flaccid bag is to allow the user to 'feel' the compliance of the patients airways. (N.B. a PEEP valve can be placed on an ambu bag). A flaccid bag requires a steady flow of oxygen or air to keep the bag inflated. Effective bag-valve mask ventilation is gained be ensuring that a proper fitting mask is placed over the patients nose and mouth. Jaw thrust should also be applied to open up the upper airways and to prevent a leak. When the bag is squeezed, the chest should rise and fall - indicating a good seal and effective airflow. Just remember to never apply too much pressure to the bag as this can cause air to enter the stomach, and could cause volutrauma and barotrauma to the lungs.  Oropharyngeal Airway The oropharyngeal airway, colloquially known as a guedels airway, is a hollow plastic tube that comes in various sizes. Its main action is to prevent the tongue from sliding back against the posterior pharyngeal wall in an unconscious person, and occluding the airway. The oropharyngeal airway is a powerful tool when used with bag-valve mask ventilation. It also acts as a bite block, and can be used to assist with oropharyngeal suctioning. To size an oropharyngeal airway - hold it besides the patient face. The flange should be aligned between the patients first incisors, and the end should be at the angle of the jaw. It is inserted by holding the airway either upside down, or at 180 degrees, and turning as you insert the airway into the mouth. Complications include damage to the hard palate, damage to teeth and gagging or vomiting.  Nasopharyngeal Airway Nasopharyngeal airways are a soft pliable plastic tube with a flange at the end. They are similar to the oropharyngeal airway, however these are more suited to patients who may still have an intact gag reflex. They can also facilitate deep suction of the pharynx. Nasopharyngeal airways are measured by folding the flange against the nare of the nostril. In a properly fitting nasopharyngeal the end should reach the ear lobe. They are inserted by applying lubricant to the tube, and gently inserting into one of the nostrils. Complications may include epistaxis, aspiration, ulceration, vomiting, sinusitis, and head injuries. Nasopharyngeal airways are absolutely contraindicated in patients with basal skull fractures! 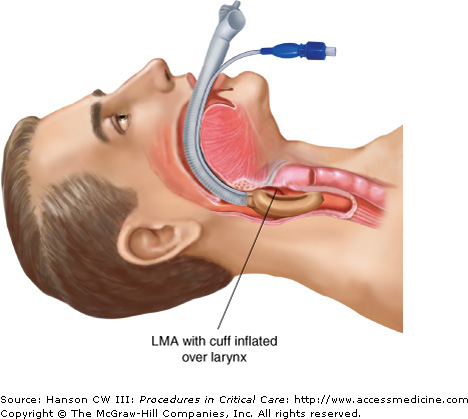 Click to see larger version! Click to see larger version! Supraglottic Airway Supraglottic airways, also known as laryngeal mask airways, are primarily used in the operating theatre settings where patients are well fasted and 'deep' enough to tolerate such a large airway device. As the name suggests the supraglottic airway consists of a 'mask' that covers the larynx and occludes the oesophagus. There are many varieties of the supraglottic airway. Some supraglottic airways have a gastric port - which provides enhanced protection from aspiration. However, aspiration is a significant risk with these airways and therefore they are contraindicated in un-fasted patients (unless it is an emergency situation). This airway cannot be used for high pressure ventilation as it can dislodge the mask and lead to air entering the stomach (therefore it is not commonly used in laparoscopic surgery). Other complications include - dislodgement, laryngospasm, coughing and sore throat, damage to teeth and aspiration. They should only be inserted by people who are trained in their use.  Endotracheal Tube The airway that we are probably most familiar with is the endotracheal tube, or ETT. The endotracheal tube is a hollow tube with a cuff at the end that is passed through the vocal cords. The cuff is inflated under the vocal cords to protect the airway from aspiration. They are very secure airways and offer the best compliance for mechanical positive pressure intubation. The bevel at the end of the tube is atraumatic - thus preventing trauma when inserting the airway. The end of the tube also has a 'murphys eye' which is a secondary opening that aims to prevent one lung ventilation. They are most commonly used in emergency situations, in un-fasted patients, and in the intensive care unit. The ETT requires skill practitioners to insert. Complications include difficult/failed intubation, trauma, bleeding, cuff perforation, endobronchial intubation (one lung ventilation) and aspirations. If the cuff at the end of the tube is inflated with too much air - this may cause necrosis of the trachea which could lead to airway stenosis (a very serious complication). A cuff manometer is recommended to ensure that the pressure in the cuff is appropriate. Stay tuned for more educational posts such as airway assessment, tracheostomies and 'cant intubate - cant ventilate'!
0 Comments
Leave a Reply. |

Nick NijkampLecturer & Registered Nurse Categories |

